
Sports Injury Rounds: 14-Year Old Gymnast with Low Back Pain
- posted: Sep. 14, 2022
Depending on the source, gymnastics is considered one of the most dangerous sports. It is not surprising that many of my sports injury patients come from this community of athletes. Not surprisingly, back pain is, by far, the most common issue I see in gymnasts. I recently treated a young athlete with a particular injury that, had it not been properly diagnosed, could have led to catastrophic consequences.
A 14-year old female gymnast entered my office with low back pain that started a month ago after doing a practice session on the balance beam. The pain was sharp at first but eased up with OTC NSAIDs and rest. But every time she went back to practicing, her back pain would return. During our initial consultation, the patient revealed that she occasionally experienced shooting pain down her right leg, but that it doesn’t last very long. Both the back pain and occasional leg pain would occur only when sleeping on her stomach, standing for long periods, or practicing gymnastics. Sitting while at school or at home was not irritating. There was no recent history of other illness.
At this point my differential diagnosis included Herniated Disc with Radiculopathy, Subacute Facet Syndrome with Sciatica, or Spondylolysis with possible Spondylolithesis. Each of these diagnoses were plausible, however, a focused exam and proper imaging were essential to narrowing down the underlying injury and choosing the correct care path. An NMS exam also included a postural exam, squat test, and flexibility evaluation. Positive findings included a slight forward lean while standing, pain in the lumbar spine during a squat, tight hip flexors, pain during P to A palpation of the lumbar spine, positive Yoeman’s Test on the right, and a positive Stork Test bilaterally. All other tests including Leseagues, Sitting Root Test, and SLR were negative. All neurological tests were WNL.
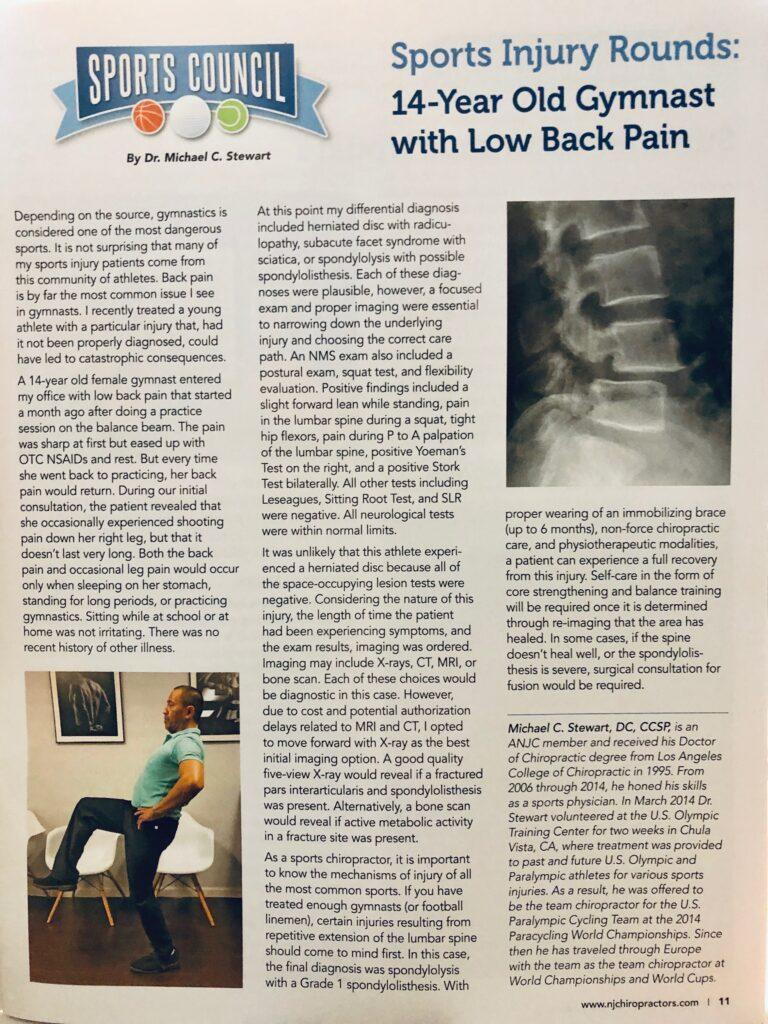
It was unlikely that this athlete experienced a herniated disc because all of the space-occupying lesion tests were negative. Considering the nature of this injury, the length of time the the patient had been experiencing symptoms, and the exam results, imaging was ordered. Imaging may include x-rays, CT, MRI, or bone scan. Each of these choices would be diagnostic in this case. However, due to costs and potential authorization delays related to MRI and CT, I opted to move forward with x-ray as the best initial imaging option. A good quality 5 view x-ray would reveal if a fractured pars interarticularis and Spondylolisthesis was present. Alternatively, a bone scan would reveal if active metabolic activity in a fracture site was present.
As a Sports Chiropractor, it is important to know the mechanisms of injury of all the most common sports. If you have treated enough gymnasts (or football linemen), certain injuries resulting from repetitive extension of the lumbar spine should come to mind first. In this case, the final diagnosis was Spondylolysis with a Grade 1 Spodylolisthesis. With proper wearing of an immobilizing brace (up to 6 months), non-force chiropractic care, and physiotherapeutic modalities, a patient can experience a full recovery from this injury. Self-care in the form of core strengthening and balance training will be required once it is determined through re-imaging that the area has healed. In some cases, if the spine doesn’t heal well, or the Spodylolisthesis is severe, surgical consultation for fusion would be required.
Published in ANJC July 2019
Stewart Sports Chiropractic & Wellness
116 Oglethorpe Professional Blvd A
Savannah, GA 31406
Office Hours
9:00 am - 6:00 pm
12:00 pm - 6:00 pm
9:00 am - 6:00 pm
Closed
9:00 am - 6:00 pm
Closed
Closed
